Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕
- Author: Alexis Thomson
- Performer: -
Book online «Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕». Author Alexis Thomson
The deformity resulting from these necessarily heroic measures is not so great as might be expected, and can be further diminished by plastic operations, which should be undertaken before cicatricial contraction has occurred.
Bed-SoresBed-sores are most frequently met with in old and debilitated patients, or in those whose tissues are devitalised by acute or chronic diseases associated with stagnation of blood in the peripheral veins. Any interference with the nerve-supply of the skin, whether from injury or disease of the central nervous system or of the peripheral nerves, strongly predisposes to the formation of bed-sores. Prolonged and excessive pressure over a bony prominence, especially if the parts be moist with skin secretions, urine, or wound discharges, determines the formation of a sore. Excoriations, which may develop into true bed-sores, sometimes form where two skin surfaces remain constantly apposed, as in the region of the scrotum or labium, under pendulous mammæ, or between fingers or toes confined in a splint.
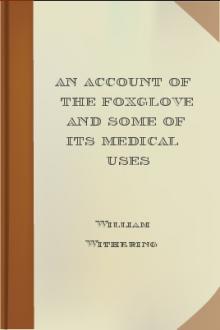
Fig. 24.—Acute Bed-Sores over Right Buttock.
Clinical Features.—Two clinical varieties are met with—the acute and the chronic bed-sore.
The acute bed-sore usually occurs over the sacrum or buttock. It develops rapidly after spinal injuries and in the course of certain brain diseases. The part affected becomes red and congested, while the surrounding parts are œdematous and swollen, blisters form, and the skin loses its vitality (Fig. 24).
In advanced cases of general paralysis of the insane, a peculiar form of acute bed-sore beginning as a blister, and passing on to the formation of a black, dry eschar, which slowly separates, occurs on such parts as the medial side of the knee, the angle of the scapula, and the heel.
The chronic bed-sore begins as a dusky reddish purple patch, which gradually becomes darker till it is almost black. The parts around are œdematous, and a blister may form. This bursts and exposes the papillæ of the skin, which are of a greenish hue. A tough greyish-black slough forms, and is slowly separated. It is not uncommon for the gangrenous area to continue to spread both in width and in depth till it reaches the periosteum or bone. Bed-sores over the sacrum sometimes implicate the vertebral canal and lead to spinal meningitis, which usually proves fatal.
In old and debilitated patients the septic absorption taking place from a bed-sore often proves a serious complication of other surgical conditions. From this cause, for example, old people may succumb during the treatment of a fractured thigh.
The granulating surface left on the separation of the slough tends to heal comparatively rapidly.
Prevention of Bed-sores.—The first essential in the prevention of bed-sores is the regular changing of the patient's position, so that no one part of the body is continuously pressed upon for any length of time. Ring-pads of wool, air-cushions, or water-beds are necessary to remove pressure from prominent parts. Absolute dryness of the skin is all-important. At least once a day, the sacrum, buttocks, shoulder-blades, heels, elbows, malleoli, or other parts exposed to pressure, must be sponged with soap and water, thoroughly dried, and then rubbed with methylated spirit, which is allowed to dry on the skin. Dusting the part with boracic acid powder not only keeps it dry, but prevents the development of bacteria in the skin secretions.
In operation cases, care must be taken that irritating chemicals used to purify the skin do not collect under the patient and remain in contact with the skin of the sacrum and buttocks during the time he is on the operating-table. There is reason to believe that the so-called “post-operation bed-sore” may be due to such causes. A similar result has been known to follow soiling of the sheets by the escape of a turpentine enema.
Treatment.—Once a bed-sore has formed, every effort must be made to prevent its spread. Alcohol is used to cleanse the broken surface, and dry absorbent dressings are applied and frequently changed. It is sometimes found necessary to employ moist or oily substances, such as boracic poultices, eucalyptus ointment, or balsam of Peru, to facilitate the separation of sloughs, or to promote the growth of granulations. In patients who are not extremely debilitated the slough may be excised, the raw surface scraped, and then painted with iodine.
Skin-grafting is sometimes useful in covering in the large raw surface left after separation or removal of sloughs.
CHAPTER VIIBACTERIAL AND OTHER WOUND INFECTIONS Erysipelas —Diphtheria —Tetanus —Hydrophobia —Anthrax —Glanders —Actinomycosis —Mycetoma —Delhi boil —Chigoe —Poisoning by insects —Snake-bites. Erysipelas
Erysipelas, popularly known as “rose,” is an acute spreading infective disease of the skin or of a mucous membrane due to the action of a streptococcus. Infection invariably takes place through an abrasion of the surface, although this may be so slight that it escapes observation even when sought for. The streptococci are found most abundantly in the lymph spaces just beyond the swollen margin of the inflammatory area, and in the serous blebs which sometimes form on the surface.
Clinical Features.—Facial erysipelas is the commonest clinical variety, infection usually occurring through some slight abrasion in the region of the mouth or nose, or from an operation wound in this area. From this point of origin the inflammation may spread all over the face and scalp as far back as the nape of the neck. It stops, however, at the chin, and never extends on to the front of the neck. There is great œdema of the face, the eyes becoming closed up, and the features unrecognisable. The inflammation may spread to the meninges, the intracranial venous sinuses, the eye, or the ear. In some cases the erysipelas invades the mucous membrane of the mouth, and spreads to the fauces and larynx, setting up an œdema of the glottis which may prove dangerous to life.
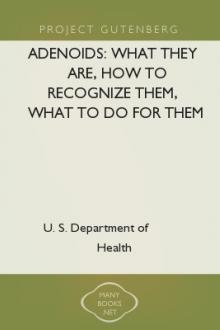
Erysipelas occasionally attacks an operation wound that has become septic; and it may accompany septic infection of the genital tract in puerperal women, or the separation of the umbilical cord in infants (erysipelas neonatorum). After an incubation period, which varies from fifteen to sixty hours, the patient complains of headache, pains in the back and limbs, loss of appetite, nausea, and frequently there is vomiting. He has a chill or slight rigor, initiating a rise of temperature to 103°, 104°, or 105° F.; and a full bounding pulse of about 100 (Fig. 25). The tongue is foul, the breath heavy, and, as a rule, the bowels are constipated. There is frequently albuminuria, and occasionally nocturnal delirium. A moderate degree of leucocytosis (15,000 to 20,000) is usually present.
Around the seat of inoculation a diffuse red patch forms, varying in hue from a bright scarlet to a dull brick-red. The edges are slightly raised above the level of the surrounding skin, as may readily be recognised by gently stroking the part from the healthy towards the affected area. The skin is smooth, tense, and glossy, and presents here and there blisters filled with serous fluid. The local temperature is raised, and the part is the seat of a burning sensation and is tender to the touch, the most tender area being the actively spreading zone which lies about half an inch beyond the red margin.
Fig. 25.—Chart of Erysipelas occurring in a wound.
The disease tends to spread spasmodically and irregularly, and the direction and extent of its progress may be recognised by mapping out the peripheral zone of tenderness. Red streaks appear along the lines of the superficial lymph vessels, and the deep lymphatics may sometimes be palpated as firm, tender cords. The neighbouring glands, also, are generally enlarged and tender.
The disease lasts for from two or three days to as many weeks, and relapses are frequent. Spontaneous resolution usually takes place, but the disease may prove fatal from absorption of toxins, involvement of the brain or meninges, or from general streptococcal infection.
Complications.—Diffuse suppurative cellulitis is the most serious local complication, and results from a mixed infection with other pyogenic bacteria. Small localised superficial abscesses may form during the convalescent stage. They are doubtless due to the action of skin bacteria, which attack the tissues devitalised by the erysipelas. A persistent form of œdema sometimes remains after recurrent attacks of erysipelas, especially when they affect the face or the lower extremity, a condition which is referred to with elephantiasis.
Treatment.—The first indication is to endeavour to arrest the spread of the process. We have found that by painting with linimentum iodi, a ring half an inch broad, about an inch in front of the peripheral tender zone—not the red margin—an artificial leucocytosis is produced, and the advancing streptococci are thereby arrested. Several coats of the iodine are applied, one after the other, and this is repeated daily for several days, even although the erysipelas has not overstepped the ring. Success depends upon using the liniment of iodine (the tincture is not strong enough), and in applying it well in front of the disease. To allay pain the most useful local applications are ichthyol ointment (1 in 6), or lead and opium fomentations.
The general treatment consists in attending to the emunctories, in administrating quinine in small—two-grain—doses every four hours, or salicylate of iron (2–5 gr. every three hours), and in giving plenty of fluid nourishment. It is worthy of note that the anti-streptococcic serum has proved of less value in the treatment of erysipelas than might have been expected, probably because the serum is not made from the proper strain of streptococcus.
It is not necessary to isolate cases of erysipelas, provided the usual precautions against carrying infection from one patient to another are rigidly carried out.
DiphtheriaDiphtheria is an acute infective disease due to the action of a specific bacterium, the bacillus diphtheriæ or Klebs-Löffler bacillus. The disease is usually transmitted from one patient to another, but it may be contracted from cats, fowls, or through the milk of infected cows. Cases have occurred in which the surgeon has carried the infection from one patient to another through neglect of antiseptic precautions. The incubation period varies from two to seven days.
Clinical Features.—In pharyngeal diphtheria, on the first or second day of the disease, redness and swelling of the mucous membrane of the pharynx, tonsils, and palate are well marked, and small, circular greenish or grey patches of false membrane, composed of necrosed epithelium, fibrin, leucocytes, and red blood corpuscles, begin to appear. These rapidly increase in area and thickness, till they coalesce and form a complete covering to the parts. In the pharynx the false membrane is less adherent to the surface than it is when the disease affects the air-passages. The diphtheritic process may spread from the pharynx to the nasal cavities, causing blocking of the nares, with a profuse ichorous discharge from the nostrils, and sometimes severe epistaxis. The infection may spread along the nasal duct to the conjunctiva. The middle ear also may become involved by spread along the auditory (Eustachian) tube.
The lymph glands behind the angle of the jaw enlarge and become tender, and may suppurate from superadded infection. There is pain on swallowing, and often earache; and the patient speaks with a nasal accent. He becomes weak and anæmic, and loses
Free e-book «Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕» - read online now



Comments (0)