Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕
- Author: Alexis Thomson
- Performer: -
Book online «Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕». Author Alexis Thomson
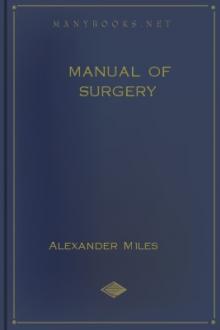
Fig. 73.—Radiogram of Innominate Aneurysm after treatment by the Moore-Corradi method. Two feet of finely drawn silver wire were introduced. The patient, a woman, æt. 47, lived for ten months after operation, free from pain (cf. Fig. 75).
Colt's method of wiring has been mainly used in the treatment of abdominal aneurysm; gilt wire in the form of a wisp is introduced through the cannula and expands into an umbrella shape.
Subcutaneous Injections of Gelatin.—Three or four ounces of a 2 per cent. solution of white gelatin in sterilised water, at a temperature of about 100° F., are injected into the subcutaneous tissue of the abdomen every two, three, or four days. In the course of a fortnight or three weeks improvement may begin. The clot which forms is liable to soften and be absorbed, but a repetition of the injection has in several cases established a permanent cure.
Amputation of the limb is indicated in cases complicated by suppuration, by secondary hæmorrhage after excision or ligation, or by gangrene. Amputation at the shoulder was performed by Fergusson in a case of subclavian aneurysm, as a means of arresting the blood-flow through the sac.
Traumatic AneurysmThe essential feature of a traumatic aneurysm is that it is produced by some form of injury which divides all the coats of the artery. The walls of the injured vessel are presumably healthy, but they form no part of the sac of the aneurysm. The sac consists of the condensed and thickened tissues around the artery.
The injury to the artery may be a subcutaneous one such as a tear by a fragment of bone: much more commonly it is a punctured wound from a stab or from a bullet.
The aneurysm usually forms soon after the injury is inflicted; the blood slowly escapes into the surrounding tissues, gradually displacing and condensing them, until they form a sac enclosing the effused blood.
Less frequently a traumatic aneurysm forms some considerable time after the injury, from gradual stretching of the fibrous cicatrix by which the wound in the wall of the artery has been closed. The gradual stretching of this cicatrix results in condensation of the surrounding structures which form the sac, on the inner aspect of which laminated clot is deposited.
A traumatic aneurysm is almost always sacculated, and, so long as it remains circumscribed, has the same characters as a pathological sacculated aneurysm, with the addition that there is a scar in the overlying skin. A traumatic aneurysm is liable to become diffuse—a change which, although attended with considerable risk of gangrene, has sometimes been the means of bringing about a cure.
The treatment is governed by the same principles as apply to the pathological varieties, but as the walls of the artery are not diseased, operative measures dealing with the sac and the adjacent segment of the affected artery are to be preferred.
Arterio-Venous AneurysmAn abnormal communication between an artery and a vein constitutes an arterio-venous aneurysm. Two varieties are recognised—one in which the communication is direct—aneurysmal varix; the other in which the vein communicates with the artery through the medium of a sac—varicose aneurysm.
Either variety may result from pathological causes, but in the majority of cases they are traumatic in origin, being due to such injuries as stabs, punctured wounds, and gun-shot injuries which involve both artery and vein. In former times the most common situation was at the bend of the elbow, the brachial artery being accidentally punctured in blood-letting from the median basilic vein. Arterio-venous aneurysm is a frequent result of injuries by modern high-velocity bullets—for example, in the neck or groin.
In aneurysmal varix the higher blood pressure in the artery forces arterial blood into the vein, which near the point of communication with the artery tends to become dilated, and to form a thick-walled sac, beyond which the vessel and its tributaries are distended and tortuous. The clinical features resemble those associated with varicose veins, but the entrance of arterial blood into the dilated veins causes them to pulsate, and produces in them a vibratory thrill and a loud murmur. In those at the groin, the distension of the veins may be so great that they look like sinuses running through the muscles, a feature that must be taken into account in any operation.
As the condition tends to remain stationary, the support of an elastic bandage is all that is required; but when the condition progresses and causes serious inconvenience, it may be necessary to cut down and expose the communication between the artery and vein, and, after separating the vessels, to close the opening in each by suture; this may be difficult or impossible if the parts are matted from former suppuration. If it is impossible thus to obliterate the communication, the artery should be ligated above and below the point of communication; although the risk of gangrene is considerable unless means are taken to develop the collateral circulation beforehand (Makins).
Varicose aneurysm usually develops in relation to a traumatic aneurysm, the sac becoming adherent to an adjacent vein, and ultimately opening into it. In this way a communication between the artery and the vein is established, and the clinical features are those of a combination of aneurysm and aneurysmal varix.
As there is little tendency to spontaneous cure, and as the aneurysm is liable to increase in size and finally to rupture, operative treatment is usually called for. This is carried out on the same lines as for aneurysmal varix, and at the same time incising the sac, turning out the clots, and ligating any branches which open into the sac. If it can be avoided, the vein should not be ligated.
ANEURYSMS OF INDIVIDUAL ARTERIESThoracic Aneurysm.—All varieties of aneurysm occur in the aorta, the fusiform being the most common, although a sacculated aneurysm frequently springs from a fusiform dilatation.
The clinical features depend chiefly on the direction in which the aneurysm enlarges, and are not always well marked even when the sac is of considerable size. They consist in a pulsatile swelling—sometimes in the supra-sternal notch, but usually towards the right side of the sternum—with an increased area of dulness on percussion. With the X-rays a dark shadow is seen corresponding to the sac. Pain is usually a prominent symptom, and is largely referable to the pressure of the aneurysm on the vertebræ or the sternum, causing erosion of these bones. Pressure on the thoracic veins and on the air-passage causes cyanosis and dyspnœa. When the œsophagus is pressed upon, the patient may have difficulty in swallowing. The left recurrent nerve may be stretched or pressed upon as it hooks round the arch of the aorta, and hoarseness of the voice and a characteristic “brassy” cough may result from paralysis of the muscles of the larynx which it supplies. The vagus, the phrenic, and the spinal nerves may also be pressed upon. When the aneurysm is on the transverse part of the arch, the trachea is pulled down with each beat of the heart—a clinical phenomena known as the “tracheal tug.” Aneurysm of the descending aorta may, after eroding the bodies of the vertebræ (Fig. 71) and posterior portions of the ribs, form a swelling in the back to the left of the spine.
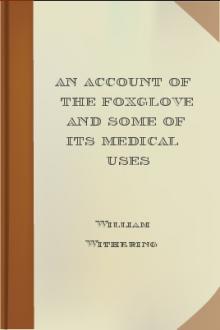
Fig. 74.—Thoracic Aneurysm, threatening to rupture externally, but prevented from doing so by Macewen's needling. The needles were left in for forty-eight hours.
Inasmuch as obliteration of the sac and the feeding artery is out of the question, surgical treatment is confined to causing coagulation of the blood in an extension or pouching of the sac, which, making its way through the parietes of the chest, threatens to rupture externally. This may be achieved by Macewen's needles or by the introduction of wire into the sac. We have had cases under observation in which the treatment referred to has been followed by such an amount of improvement that the patient has been able to resume a laborious occupation for one or more years. Christopher Heath found that improvement followed ligation of the left common carotid in aneurysm of the transverse part of the aortic arch.
Abdominal Aneurysm.—Aneurysm is much less frequent in the abdominal than in the thoracic aorta. While any of the large branches in the abdomen may be affected, the most common seats are in the aorta itself, just above the origin of the cœliac artery and at the bifurcation.
The clinical features vary with the site of the aneurysm and with its rapidity and direction of growth. A smooth, rounded swelling, which exhibits expansile pulsation, forms, usually towards the left of the middle line. It may extend upwards under cover of the ribs, downwards towards the pelvis, or backward towards the loin. On palpation a systolic thrill may be detected, but the presence of a murmur is neither constant nor characteristic. Pain is usually present; it may be neuralgic in character, or may simulate renal colic. When the aneurysm presses on the vertebræ and erodes them, the symptoms simulate those of spinal caries, particularly if, as sometimes happens, symptoms of compression paraplegia ensue. In its growth the swelling may press upon and displace the adjacent viscera, and so interfere with their functions.
The diagnosis has to be made from solid or cystic tumours overlying the artery; from a “pulsating aorta”; and from spinal caries; much help is obtained by the use of the X-rays.
The condition usually proves fatal, either by the aneurysm bursting into the peritoneal cavity, or by slow leakage into the retro-peritoneal tissue.
The Moore-Corradi method has been successfully employed, access to the sac having been obtained by opening the abdomen. Ligation of the aorta has so far been unsuccessful, but in one case operated upon by Keen the patient survived forty-eight days.
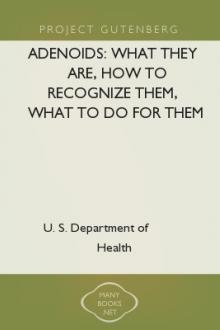
Innominate aneurysm may be of the fusiform or of the sacculated variety, and is frequently associated with pouching of the aorta. It usually grows upwards and laterally, projecting above the sternum and right clavicle, which may be eroded or displaced (Fig. 75). Symptoms of pressure on the structures in the neck, similar to those produced by aortic aneurysm, occur. The pulses in the right upper extremity and in the right carotid and its branches are diminished and delayed. Pressure on the right brachial plexus causes shooting pain down the arm and muscular paresis on that side. Vaso-motor disturbances and contraction of the pupil on the right side may result from pressure on the sympathetic. Death may take place from rupture, or from pressure on the air-passage.
Fig. 75.—Innominate Aneurysm in a woman, æt. 47, eight months after treatment by Moore-Corradi method (cf. Fig. 73).
The available methods of treatment are ligation of the right common carotid and third part of the right subclavian (Wardrop's operation), of which a number of successful cases have been recorded. Those most suitable for ligation are cases in which the aneurysm is circumscribed and globular (Sheen). If ligation is found to be impracticable, the Moore-Corradi method or Macewen's needling may be tried.
Carotid Aneurysms.—Aneurysm of the common carotid is more frequent on the right than on the left side, and is usually situated either at the root of the neck or near the bifurcation. It is the aneurysm most frequently met with in women. From its position the swelling is liable to press on the vagus, recurrent and sympathetic nerves, on the air-passage, and on the œsophagus, giving rise to symptoms referable to such pressure. There may be cerebral symptoms from interference with the blood supply of the brain.
Aneurysm near the origin has to be diagnosed from subclavian, innominate, and aortic aneurysm, and from other swell
Free e-book «Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕» - read online now



Comments (0)