Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕
- Author: Alexis Thomson
- Performer: -
Book online «Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕». Author Alexis Thomson
Tuberculous disease in the glands of the groin is comparatively rare. We have chiefly observed it in the femoral glands as a result of inoculation tubercle on the toes or sole of the foot. The affected glands nearly always break down and suppurate, and after destroying the overlying skin give rise to fungating ulcers. The treatment consists in excising the glands and the affected skin. The dissection may be attended with troublesome hæmorrhage from the numerous veins that converge towards the femoral trunk.
Tuberculous disease in the mesenteric and bronchial glands is described with the surgery of regions.
Syphilitic Disease of Glands.—Enlargement of lymph glands is a prominent feature of acquired syphilis, especially in the form of the indolent or bullet-bubo which accompanies the primary lesion, and the general enlargement of glands that occurs in secondary syphilis. Gummatous disease in glands is extremely rare; the affected gland rapidly enlarges to the size of a walnut, and may then persist for a long period without further change; if it breaks down, the overlying skin is destroyed and the caseated tissue of the gumma exposed.
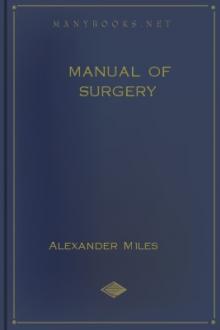
Lymphadenoma.—Hodgkin's Disease (Pseudo-leukæmia of German authors).—This is a rare disease, the origin of which is as yet unknown, but analogy would suggest that it is due to infection with a slowly growing micro-organism. It is chiefly met with in young subjects, and is characterised by a painless enlargement of a particular group of glands, most commonly those in the cervical region (Fig. 80).
Fig. 80.—Chronic Hodgkin's Disease in a boy æt. 11.
The glands are usually larger than in tuberculosis, and they remain longer discrete and movable; they are firm in consistence, and on section present a granular appearance due to overgrowth of the connective-tissue framework. In time the glandular masses may form enormous projecting tumours, the swelling being added to by lymphatic œdema of the overlying cellular tissue and skin.
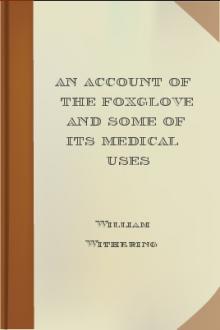
The enlargement spreads along the chain of glands to those above the clavicle, to those in the axilla, and to those of the opposite side (Fig. 81). Later, the glands in the groin become enlarged, and it is probable that the infection has spread from the neck along the mediastinal, bronchial, retro-peritoneal, and mesenteric glands, and has branched off to the iliac and inguinal groups.
Two clinical types are recognised, one in which the disease progresses slowly and remains confined to the cervical glands for two or more years; the other, in which the disease is more rapidly disseminated and causes death in from twelve to eighteen months.
Fig. 81.—Lymphadenoma (Hodgkin's Disease) affecting left side of neck and left axilla, in a woman æt. 44. Three years' duration.
In the acute form, the health suffers, there is fever, and the glands may vary in size with variations in the temperature; the blood presents the characters met with in secondary anæmia. The spleen, liver, testes, and mammæ may be enlarged; the glandular swellings press on important structures, such as the trachea, œsophagus, or great veins, and symptoms referable to such pressure manifest themselves.
Diagnosis.—Considerable difficulty attends the diagnosis of lymphadenoma at an early stage. The negative results of tuberculin tests may assist in the differentiation from tuberculous disease, but the more certain means of excising one of the suspected glands and submitting it to microscopical examination should be had recourse to. The sections show proliferation of endothelial cells, the formation of numerous giant cells quite unlike those of tuberculosis and a progressive fibrosis. Lympho-sarcoma can usually be differentiated by the rapid assumption of the local features of malignant disease, and in a gland removed for examination, a predominance of small round cells with scanty protoplasm. The enlargement associated with leucocythæmia is differentiated by the characteristic changes in the blood.
Treatment.—In the acute form of lymphadenoma, treatment is of little avail. Arsenic may be given in full doses either by the mouth or by subcutaneous injection; the intravenous administration of neo-salvarsan may be tried. Exposure to the X-rays and to radium has been more successful than any other form of treatment. Excision of glands, although sometimes beneficial, seldom arrests the progress of the disease. The ease and rapidity with which large masses of glands may be shelled out is in remarkable contrast to what is observed in tuberculous disease. Surgical interference may give relief when important structures are being pressed upon—tracheotomy, for example, may be required where life is threatened by asphyxia.
Leucocythæmia.—This is a disease of the blood and of the blood-forming organs, in which there is a great increase in the number, and an alteration of the character, of the leucocytes present in the blood. It may simulate lymphadenoma, because, in certain forms of the disease, the lymph glands, especially those in the neck, axilla, and groin, are greatly enlarged.
Tumours of Lymph GlandsPrimary Tumours.—Lympho-sarcoma, which may be regarded as a sarcoma starting in a lymph gland, appears in the neck, axilla, or groin as a rapidly growing tumour consisting of one enlarged gland with numerous satellites. As the tumour increases in size, the sarcomatous tissue erupts through the capsule of the gland, and infiltrates the surrounding tissues, whereby it becomes fixed to these and to the skin.
Fig. 82.—Lympho-Sarcoma removed from Groin. It will be observed that there is one large central parent tumour surrounded by satellites.
The prognosis is grave in the extreme, and the only hope is in early excision, followed by the use of radium and X-rays. We have observed a case of lympho-sarcoma above the clavicle, in which excision of all that was removable, followed by the insertion of a tube of radium for ten days, was followed by a disappearance of the disease over a period which extended to nearly five years, when death resulted from a tumour in the mediastinum. In a second case in which the growth was in the groin, the patient, a young man, remained well for over two years and was then lost sight of.
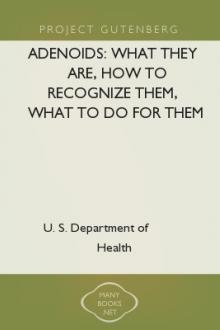
Secondary Tumours.—Next to tuberculosis, secondary cancer is the most common disease of lymph glands. In the neck it is met with in association with epithelioma of the lip, tongue, or fauces. The glands form tumours of variable size, and are often larger than the primary growth, the characters of which they reproduce. The glands are at first movable, but soon become fixed both to each other and to their surroundings; when fixed to the mandible they form a swelling of bone-like hardness; in time they soften, liquefy, and burst through the skin, forming foul, fungating ulcers. A similar condition is met with in the groin from epithelioma of the penis, scrotum, or vulva. In cancer of the breast, the infection of the axillary glands is an important complication.
In pigmented or melanotic cancers of the skin, the glands are early infected and increase rapidly, so that, when the primary growth is still of small size—as, for example, on the sole of the foot—the femoral glands may already constitute large pigmented tumours.
Fig. 83.—Cancerous Glands in Neck secondary to Epithelioma of Lip.
(Mr. G. L. Chiene's case.)
The implication of the glands in other forms of cancer will be considered with regional surgery.
Secondary sarcoma is seldom met with in the lymph glands except when the primary growth is a lympho-sarcoma and is situated in the tonsil, thyreoid, or testicle.
CHAPTER XVITHE NERVES Anatomy —Injuries of Nerves: Changes in nerves after division; Repair and its modifications; Clinical features; Primary and secondary suture —Subcutaneous Injuries of Nerves —Diseases: Neuritis; Tumours —Surgery of the individual nerves: Brachial neuralgia; Sciatica; Trigeminal neuralgia.
Anatomy.—A nerve-trunk is made up of a variable number of bundles of nerve fibres surrounded and supported by a framework of connective tissue. The nerve fibres are chiefly of the medullated type, and they run without interruption from a nerve cell or neuron in the brain or spinal medulla to their peripheral terminations in muscle, skin, and secretory glands.
Each nerve fibre consists of a number of nerve fibrils collected into a central bundle—the axis cylinder—which is surrounded by an envelope, the neurolemma or sheath of Schwann. Between the neurolemma and the axis cylinder is the medullated sheath, composed of a fatty substance known as myelin. This medullated sheath is interrupted at the nodes of Ranvier, and in each internode is a nucleus lying between the myelin and the neurolemma. The axis cylinder is the essential conducting structure of the nerve, while the neurolemma and the myelin act as insulating agents. The axis cylinder depends for its nutrition on the central neuron with which it is connected, and from which it originally developed, and it degenerates if it is separated from its neuron.
The connective-tissue framework of a nerve-trunk consists of the perineurium, or general sheath, which surrounds all the bundles; the epineurium, surrounding individual groups of bundles; and the endoneurium, a delicate connective tissue separating the individual nerve fibres. The blood vessels and lymphatics run in these connective-tissue sheaths.
According to Head and his co-workers, Sherren and Rivers, the afferent fibres in the peripheral nerves can be divided into three systems:—
Those which subserve deep sensibility and conduct the impulses produced by pressure as well as those which enable the patient to recognise the position of a joint on passive movement (joint-sensation), and the kinæsthetic sense, which recognises that active contraction of the muscle is taking place (active muscle-sensation). The fibres of this system run with the motor nerves, and pass to muscles, tendons, and joints. Even division of both the ulnar and the median nerves above the wrist produces little loss of deep sensibility, unless the tendons are also cut through. The failure to recognise this form of sensibility has been largely responsible for the conflicting statements as to the sensory phenomena following operations for the repair of divided nerves.
Those which subserve protopathic sensibility—that is, are capable of responding to painful cutaneous stimuli and to the extremes of heat and cold. These also endow the hairs with sensibility to pain. They are the first to regenerate after division.
Those which subserve epicritic sensibility, the most highly specialised, capable of appreciating light touch, e.g. with a wisp of cotton wool, as a well-localised sensation, and the finer grades of temperature, called cool and warm (72°–104° F.), and of discriminating as separate the points of a pair of compasses 2 cms. apart. These are the last to regenerate.
A nerve also exerts a trophic influence on the tissues in which it is distributed.
The researches of Stoffel on the minute anatomy of the larger nerves, and the disposition in them of the bundles of nerve fibres supplying different groups of muscles, have opened up what promises to be a fruitful field of
Free e-book «Manual of Surgery by Alexis Thomson (golden son ebook .TXT) 📕» - read online now



Comments (0)